Table of ContentsWho - Health Policy - TruthsThe 8-Minute Rule for Healthcare Policies - List Of High Impact Articles - Ppts ...The Single Strategy To Use For Who - Health PolicyThe Health Care Policy - Jama Network IdeasThe smart Trick of United States - Commonwealth Fund That Nobody is DiscussingHow 8 Health Care Regulations In United States - Regis College can Save You Time, Stress, and Money.
Contrast nations are Australia, New Zealand, Spain, South Africa, Switzerland, and the UK. Rate information are not available for all items and services in all nations (e.g., prices for Xarelto are readily available just for South Africa, Spain, Switzerland, the UK, and the United States, not for Australia or New Zealand).
average for all 21 and are the greatest amongst all the countries (that is, the U.S. average exceeds the non-U.S. optimum) for 18. Balanced throughout the non-U.S. mean rates, costs in the United States are more than twice as high as costs in peer nations. And even when averaged across the non-U.S.
costs are more than 40 percent higher. Significantly, a variety of these products and services are highly tradeableparticularly pharmaceuticals. The truth that international tradeability has actually not deteriorated massive cost differentials in between the United States and other countries ought to be a red flag that something noticeably ineffective is happening in the U.S.
The Main Principles Of Health Care For All: A Framework For Moving To A Primary Care ...
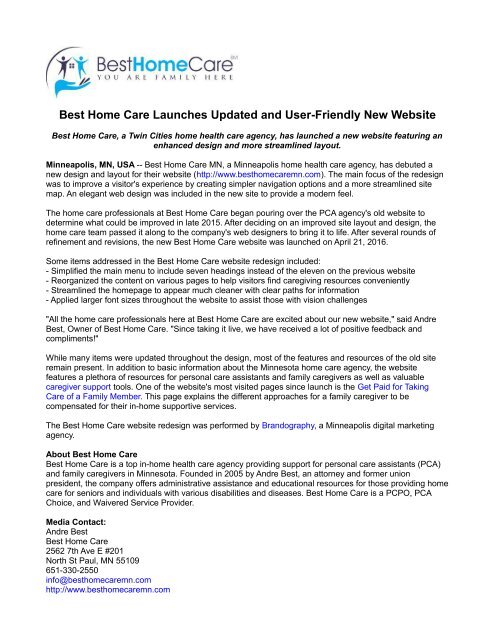
shows some specific measures of usage that correspond to the rate data highlighted in Figure L: the occurrence of angioplasties, appendectomies, cesarean areas, hip replacements, and knee replacements, normalized by the size of the nation's population. On two of the 5 measures, the United States has either a normal (angioplasties) or fairly low (appendectomies) utilization rate relative to other nations' averages.
For all four of these procedures, the United States is well listed below the highest usage rate. The United States is only the highest-utilization countryby a small marginwhen it comes to knee replacements. In brief, if one were looking just at the data charting health care utilization, one would have little reason to guess that the United States invests far more than its innovative nation peers on healthcare.
OECD minimum OECD optimum 30-OECD-peer-country average 1 Angioplasty 0.19 2.15 1.03 Appendectomy 0.79 2.03 1.39 C-section 0.41 1.92 0.76 Hip replacement 0.12 1.49 0.76 Knee replacement 0.03 0.93 0.47 1 ChartData Download data The data underlying the figure. Utilization steps are normalized by population. U.S. levels are set at 1, and procedures of utilization for other countries are indexed relative to the U.S.
Some Known Factual Statements About The National Academy For State Health Policy
Author's analysis of OECD 2018a reveals another set of global comparisons of healthcare inputs and rates, from Laugesen and Glied (2008 ). Laugesen and Glied compare doctor services' utilization and salaries in Australia, Canada, France, Germany, and the UK with those in the United States (in the figure, the U.S.
They find that utilization of primary care physicians by patients is greater in all of these nations, by an average of more than half. Yet wages of primary care physicians are higher in the U.S., by approximately half. The usage measure they utilize for orthopedists is hip replacements.
They are roughly as typical in Australia (94 to 100) and the United Kingdom (105 to 100), and they are more typical in France and Germany. Orthopedist incomes are much higher in the United States than in any peer countrymore than twice as high on average. The income comparisons in Figure N are net of doctor's debt service payments for medical school loans, so this common explanation for high American doctor incomes can not describe these distinctions.
The smart Trick of Health Care Policy - Boundless Political Science That Nobody is Discussing
= 1 Medical care doctors' wages Orthopedists' salaries 1 Australia 0.50 0.42 Canada 0.67 0.47 France 0.51 0.35 Germany 0.71 0.46 UK 0.86 0.73 Non-U.S. typical 0.65 0.49 1 The data underlying the figure. U.S. = 1 Primary care usage Hip replacement usage 1 Australia 1.61 0.94 Canada 1.53 0.74 France 1.84 1.33 Germany 1.95 1.67 UK 1.34 1.05 Non-U.S.
Utilization steps are stabilized by population. U.S (a health care professional is caring for a patient who is about to begin taking losartan). levels are set at 1, and procedures of utilization for other countries are indexes relative to the U.S. The information source uses incidence of hip replacements as the relative utilization measure for orthopedists. Data from Laugesen and Glied 2008 As we have kept in mind, many truly argue that most Americans would not wish to trade the healthcare offered to them today for what was offered in years past, even as main cost information show that all that has changed is the price.

This healthcare available abroad is far more affordable and TransForMationsTreatment yet of a minimum of as high quality. The fairly low level of usage and extremely high price levels in the U.S. offer suggestive proof that the faster rate of health care costs development in the United States in current decades has been driven on the price side also.
The Single Strategy To Use For Who - Health Policy
It is clear that the United States is an outlier in global comparisons of healthcare costs. It is also clear that the United States is an outlier not due to the fact that of overuse of health care however due to the fact that of the high cost of its health care. As gone over above, the United States is extremely unremarkable on health outcome measures (see Figure D) and is even toward the low end of many important health measures.
than in the vast bulk (18 of 21) of peer countries. All of this evidence highly suggests that getting U.S. health care rates more in line with international peers could have considerable success in relieving the pressure that rising healthcare costs are placing on American incomes. Even though many health researchers have actually kept in mind that pricenot utilizationis the clear source of the dysfunction of the American health system, it stands out just how much attention has been paid to decreasing usage, instead of reducing costs, when it pertains to making health policy in the United States in recent decades.
2009) to claim that as much as a third of American health spending was wasteful; hence, they concluded, terrific chances was plentiful to squeeze out this waste by targeting lower usage. what is a health care deductible. These findings were a great source of temptation for policymakers, and they were extremely influential in the American policy dispute in the run-up to the ACA.
Examine This Report on Health Care Policy - Boundless Political Science
The most apparent problem was how to build policy levers to precisely target which third of health care spending was inefficient. Even more, subsequent research study in the last few years has highlighted extra reasons to think that the Dartmouth findings would be tough to translate into policy suggestions. The earlier Dartmouth Atlas findings were mostly obtained from looking at local variation in spending by Medicare.
The authors of the Atlas hypothesized that local differences in physician practice drove cost differentials that were not associated with quality enhancements. Policymakers and analysts have frequently made the argument that if the lower-priced, however similarly effective, practices of more efficient regions might be adopted nationwide, then a large piece of inefficient costs could be ejected of the system (how much do home health care agencies charge).
Even more, Cooper et al. (2018) research study the local variation in costs on privately insured clients and discover that it does not associate tightly at all with Medicare spending. This finding calls into question the hypothesis that regional variation in practice is driving patterns in both spending and quality, as these type of region-specific practices need to affect both Medicare and private insurance coverage payments.